Empower, don’t blame the parents - Why building resilience can help parents provide their children with a healthier diet.
Author: Liz Barnes interviewing Dr Matthew Wood, author of original article
Have you ever wondered why some children develop a healthy appetite for fruit and vegetables whereas others develop a strong aversion? Is it the way that fruit and veg are introduced or when? Could it be the frequency/quality and does this link to financial considerations? Or does it relate to parenting style and the type of resilience that parents exhibit when they encounter the inevitable resistance from a child facing a healthy portion of vegetables?
Dr. Matt Wood and Professor Paurav Shukla have been researching resilience, parenting style, and children’s eating behaviours for several years and have made some surprising discoveries.
I had the pleasure of interviewing Matt following his recent academic publication in Social Marketing Quarterly. [1]

Q. Your article really got me thinking about how I tried to ‘train’ my three (now adult) children to eat fruit and veg. They delight in telling stories to their friends about the tactics I used, from bribing to coercion – as well as ensuring that I dished veg up at every meal. I’m not sure if this was my resilience or desperation – so firstly, can you explain a bit more about resilience which underpins a lot of your research?
A. The good news is that academics now widely acknowledge the role of resilience for social marketing and behaviour change [2]. It is important because instead of taking the mistaken view that knowledge will lead to action, building resilience can help empower people to make positive changes. So rather than blaming individuals for poor choices/behaviours, helping people to learn [3] resilience can build that all-important bridge between knowledge and action.
Q. So how is resilience defined?
A. Resilience refers to an individual or family’s ability to overcome adversity or life challenges and “bounce back” [4]. Building resilience means helping people, communities, countries and global institutions prevent, anticipate, prepare for, cope with and recover from adversity not only ‘bounce back’ to where they were previously but become stronger [5]. We can look at the detailed constructs of resilience later.
Q. I find this interesting because when my resilience was being ‘tested’ in different ways by my children, I was sometimes more concerned about their relationship with food rather than its nutritional value. Was I right to be just as concerned about self-esteem and positive mental health?
A. Yes, the main motivation for parents to seek help for their obese child is a concern for their child’s psychological well-being [6], There are a lot of studies which show that building parental resilience is a significant strategy to help reduce and prevent childhood obesity. Rather than a focus on weight, some argue that the focus should be on building resilience, self-esteem and the psychological aspects of obesity, because of the link to lower weight status [7].
Q. How does resilience relate to eating and feeding behaviour?
A. Parents who are overweight or obese are more likely to have overweight children [8]. As we know, healthy eating/weight isn’t determined purely by buying nutritious food or understanding what a ‘healthy diet’ is. A parent’s ability to ensure their child has a healthy diet/weight is dependent on their resilience and how well equipped they are to support their children, guiding them toward healthy eating choices and practices.
Previous research showed a positive relationship between resilience and obesity [9]. To enable better feeding practices for their children, parents may benefit from interventions that increase resilience. When more emotionally equipped, parents are more likely to apply any increased awareness of healthy eating practices for their children.
Our paper demonstrates the importance of effective interactions between parents and children for healthy eating behaviours.
Q. But resilience isn’t just about the individual’s psychological factors is it?
A. No, I’m a keen advocate of the whole systems approach; the role of social marketing to gain an understanding of what services, facilities, and networks parents have access to, and how this can impact their resilience. So rather than just thinking about the characteristics of individuals, we need to look at the sociological environment and multiple systems that they interact within enabling them to develop resilience or not. Researchers now recognise that resilience is not an individual characteristic but a product of the environment in which a person learns to cope with adversity [10].
Q. So looking at the bigger picture, we need to take account of the various pressures, lifestyles, working patterns, housing, finance, etc when considering parental resilience to feeding behaviours.
I remember that sometimes mealtimes felt like a battleground; everything I knew about nutritious feeding, just got DITCHED because I was trying to manage a difficult day within my busy schedule. Is this typical?
A. You are definitely not alone, despite a lot of education, advice and some great healthy eating for kids campaigns. We now have the benefit of lessons learned from the Change4Life programme which did increase parents’ awareness of healthy eating practices. Sadly, it failed to achieve its aim of stopping the rise of childhood obesity [11]. Practical advice to parents was successfully provided by the programme but it failed to help develop the emotional and psychological skills, or resilience, necessary to apply his knowledge.
It was clear from the initial insight gathered for Chage4Life, that there were challenges in managing family meals, for example, not eating as a family or trying to adjust for tastes by making different meals for different family members (usually containing no vegetables) [12]. Parents have the most important role in creating the environment in which children consume and experience food [13].
So this is where parenting style comes in, which we know can have a significant impact on feeding practices within a family [14]. It is illustrated by the fact that overweight parents are more likely to have overweight children [15].
Q. So I’m now starting to wonder if I had the best parenting style when it came to feeding behaviours? Can you tell me more about them?
A. It’s about how a parent interacts with their children. The three commonly defined styles are:
1. Authoritarian (high control, low warmth)
2. Authoritative (high control, high warmth)
3. Permissive (low control, high OR low warmth) [16]
The style you adopt can either help or hinder the practices you deploy as a parent.
Q. What examples are there which relate to healthy feeding practice?
A. There are quite a few studies – here are some key points:
1. Weight and obesity
- Children of authoritative mothers had the lowest risk of obesity whereas children of authoritarian mothers had the highest
- Children of permissive mothers were twice as likely to be overweight than those with an authoritative mother [17]
- Adolescents with authoritative parents had the healthiest food consumption [18].
2. Feeding practices (includes perceived responsibility, concern about weight, restriction, the pressure to eat, monitoring)
- Authoritative parents tend to demonstrate low levels of concern regarding their child’s weight and are much more likely to plan healthy family meals in advance
- Families with authoritative parents are more likely to hold positive attitudes toward healthy eating and family meal occasions.
This confirms the studies which show that there is healthier food consumption (e.g. fresh fruit and veg) when eating regular family meals and a lower risk of obesity [19]. Another example that there is a 12% reduction in the chance of a younger child becoming overweight when they eat with their family at least three meals a week [20].
Q. Did this research help you define which areas to test?
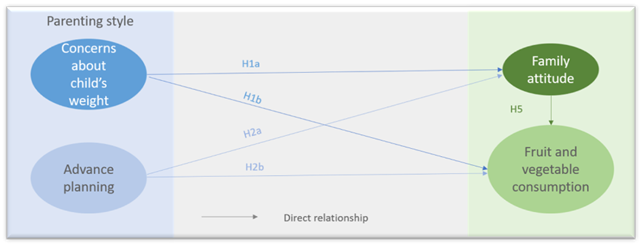
A. Yes, I’ll show you in a diagram, our two hypotheses based on parenting styles (we tested certain factors within the overall parenting style construct, which previous research had shown to be particularly significant) along with our final one about family attitude:
Hypothesis 1: Concerns about a child’s weight will be associated with (a) the family attitude toward healthy eating and (b) consumption of fruits and vegetables.
Hypothesis 2: Advanced meal planning will be associated with (a) the family attitude toward healthy eating and (b) consumption of fruits and vegetables.
Hypothesis 5: Family attitude toward healthy eating will be associated with consumption of fruits and vegetables.
Q. This feels fairly straightforward so far, but I know that you wanted to understand the influence of parental resilience on the relationship between parenting style and eating behaviour. But before you show us how you did that; can you tell give us more detail about the constructs of parental resilience?
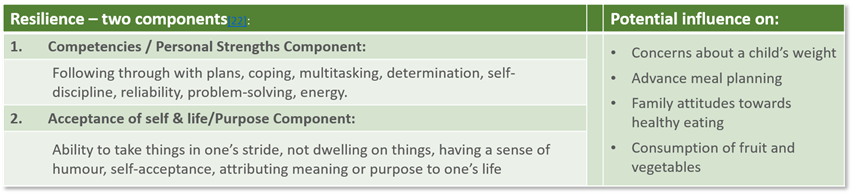
A. Research shows that resilient adults are able to adapt successfully to stress and anxiety and are often characterized by high levels of morale, optimism, forgiveness, self-efficacy, and a sense of coherence [21].
This has been subdivided into two constructs, each with their own characteristics. We can think about how these characteristics may relate to concerns about a child’s weight, advance meal planning and family attitudes towards healthy eating.
Q. What hypotheses did this present and how does this fit with your conceptual model?
A. Hypothesis 3: The personal competence aspect of parental resilience will moderate [affect the strength of] the relationship between H3a concerns about a child’s weight and consumption of fruits and vegetables and H3b advanced meal planning and consumption of fruits and vegetables.
Hypothesis 4: Acceptance of self and life aspect of parental resilience will moderate [affect the strength of] the relationship between H4a concerns about a child’s weight and consumption of fruits and vegetables and H4b advanced meal planning and consumption of fruits and vegetables.
Q. How did you go about testing this? What was your methodology?
A. We used a quantitative survey with a convenience sample of 242 parents using after-school clubs in a city on the South coast of England. The sample covered a wide spectrum of schools from those graded by Ofsted as ‘needing improvement’ to ‘excellent’.
The resilience of parents was measured on Wagnild and Young’s Resilience Scale [23] and Parenting style was captured through two factors: concern about the child’s weight [24] and advanced planning [25]. The family attitude about fruits and vegetables was captured through items derived from the study by Cullen et al. (2000). Parents also reported on actual consumption of vegetable and fruit along with the frequency of family meals. A full regression model was applied to test the relationships between the variables.
Further details about the scale, constructs, items, and sample can be found in the original article.
Q. So what did you find? Were there any surprises?
A. Let’s look at specific results: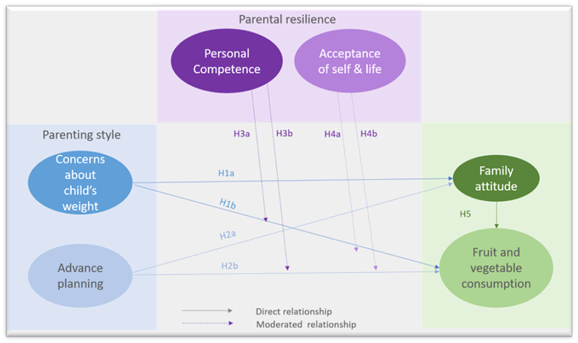
H1a - Concern about a child’s weight is positively associated with family attitudes toward fruits and vegetables but H1b shows a negative association to the child’s weekly consumption of fruits and vegetables. This demonstrates the relationship between parenting style and children’s eating behaviors. A parent can be worried about a child’s weight, but this doesn’t necessarily translate into healthy feeding behaviours.
This negative association corroborates with a rich stream of research on the attitude-behavior gap in healthy eating behaviours. [26] It also upholds earlier research which shows a discrepancy between stated attitudes and actual behaviours about healthy eating [27].
Parents may be overly concerned about their child’s weight but lack appropriate parenting skills to support them to eat more healthily.
H2a – Regarding advanced planning, this is negatively associated with family attitudes toward fruits and vegetables but H2b show a positive association between advance planning and the child’s weekly consumption of fruits and vegetables. Initially, this was a surprise as it appeared to contradict some of our previous research [28]. This can probably be explained by the fact that meal planners and food diaries may have a negative impact on one’s own eating behaviour (original research used self-reporting) but assist in the eating behaviours of one’s children [29].
H3a – There is a significant influence of personal competence on the relationship between concerns about a child’s weight and consumption of fruit and vegetables. The more competent you are, the more likely you are to feed your children fruit and veg, irrespective of your concern for their weight.
H4b – Interestingly, the acceptance of self and life component of parental resilience has a significant moderating influence on the relationship between the advance planning of healthy meals among parents and a child’s weekly consumption of fruits and vegetables. This is not surprising because these items are more concerned with optimism and general positivity rather than the planning and coping skills measured by the personal competence factor.
These results demonstrate the relationship between resilience, parenting style, and healthy eating behaviors among children. It also supports evidence from literature about resilience and obesity along with the links of a healthier diet/lower risk of childhood obesity with the traits of an authoritative parenting style. In other words, if an authoritative parenting style is underpinned by higher parental resilience, then there is a greater probability of children eating a healthy diet and a lower incidence of childhood obesity.
Q. How does this help us think about which factors to focus on regarding parental feeding behaviours?
A. The good news is that these findings help explain why higher resilience in parents is linked to healthier weight status in children [30] so we really need to understand resilience in order to develop social marketing/behaviour change interventions that focus on the how parents enable and encourage their children to eat healthily alongside what they feed children.
Q. And presumably this also links to how we can help prevent or reduce childhood obesity?
A. Yes, this study certainly suggests that building parental resilience could be effective. As we know, the feeding practices of an authoritative parenting style generally lead to higher fruit and vegetable consumption amongst children which could give rise to a reduction in the likelihood of childhood obesity. Because a relationship exists between increased resilience and the adoption of child feeding practices associated with an authoritative parenting style – the focus should be on improving resilience.
Q. So this poses an interesting sociological viewpoint about how we approach the challenge - considering a wider approach to look at external factors of resilience as well as internal?
A. That is so true – let’s break it down by looking at the personal level and the environment.
Personal level: Parents are mostly concerned about their child’s psychological well-being [31] when they are overweight and this often causes them to seek help, so we need to continue with interventions that support this. For example, as part of a child’s healthcare plan, GPs and community health workers could assess parental resilience. Appropriate support could then be offered.
Environmental level: We will need to understand which external factors are influencing resilience levels and what impact this is having on parenting style to be able to provide appropriate support.
Q. This brings us back to the systems approach to social marketing then?
A. Yes, our study supports the argument that we need to build long-term solutions, considering the environmental aspects of ‘problem’ behaviors (such as poor diet). There will be different perceived barriers/costs/benefits amongst different groups of parents so tailored interventions and different approaches will be needed to help parents adopt more effective parenting style/feeding practices.
Q. I guess this means more research is needed?
A. Social marketing must help further understand the barriers which prevent parents from enabling a healthy diet for their children. We also need to know more about the interactions of parents and children, particularly parental resilience to withstand pressures regarding children eating unhealthy food.
“This study helps social marketers understand the interactions between parents and children (and indeed, families and service providers) and—critically—to appreciate that downstream social marketing alone cannot deal effectively with a “wicked problem” like obesity.” [32]
Of course, we also make recommendations for further studies, samples, and interactions along with considering how other components of parenting style may impact child feeding practices. You can find these in our full paper.
Q. So how would you sum this up?
A. This study found that parental resilience is positively associated with behaviors and actions but not to attitudes. A social marketing approach needs to look at the whole system, how the environment impacts a parent’s resilience as well as supporting them individually in their child feeding practice.
A public health intervention that doesn’t place sole blame on the parents or isolate obese children should reflect the socioecological reasons behind parental child feeding behaviour.
Author Biographies:
Matthew Wood is principal lecturer in marketing at Brighton Business School, where he is head of the
marketing subject group. He has presented papers and keynote speeches at leading marketing conferences
and regularly publishes work in social marketing, health and medical journals.
Paurav Shukla is professor of marketing at Southampton Business School, where he is head of digital
and data driven management department. He has written in the area of customer expectations and
consumption experiences, luxury marketing and branding, public health, international marketing and
SME management in international journals.
Footnotes:
[1] Wood and Shukla 2019
[2] Wood 2018
[3] Place, Reynold, Cousins, and O’Neill 2002
[4] Masten & Coatsworth, 1998.
[5] Fan, Pandya-Lorch, & Yosef, 2014
[6] Twiddy, Wilson, Bryant, and Rudolf 2012
[7] (Birch and Davison, 2001; Stewart-Knox, Duffy and Bunting, 2012; Walker Lowry, Sallinen, & Janicke, 2007
[8] Danielzik, Czerwinski-Mast, Langna¨se, & Mu¨ller, 2004
[9] Ball et al 2002
[10] Ungar, 2008; Wood, 2018
[11] Croker et al., 2012; DOH, 2010
[12] DOH 2010
[13] Birch & Fisher, 1998
[14] Ventura & Birch, 2008
[15] Danielzik, Czerwinski-Mast, Langna¨se, & Mu¨ller, 2004
[16] Hubbs-Tait, Kennedy, Page, Topham, & Harrist, 2008
[17] Rhee, Lumeng, Appugliese, Kaciroti, and Bradley 2006
[18] Pearson, Atkin, Biddle, Gorley, & Edwardson, 2010
[19] Fruh, Fulkerson, Mulekar, Kendrick, & Clanton, 2011
[20] Hammons & Fiese, 2011
[21] McMillan and Reed, 1993; Broyles, 2005; Nygren et al., 2005; Hardy, Concato, & Gill, 2004
[22] Wagnild 2009 and Wagnild and Young 1993
[23] Wagnild and Young’s 1993
[24] Hubbs-Tait et al., 2008
[25] Cullen et al. 2000
[26] Shaw, McMaster, & Newholm, 2015.
[27] Wood & Shukla, 2016.
[28] Wood and Shukla 2016
[29] Wood and Shukla’s 2016
[30] Ball et al., 2012
[31] Twiddy, Wilson, Bryant, & Rudolf, 2012
[32] Wood and Shukla 2019
Full reference list
Ball, K., Brown, W., & Crawford, D. (2002). Who does not gain weight? Prevalence and predictors of weight maintenance in young women. International Journal of Obesity, 27, 1570–1578.
Ball, K., Cleland, V., Salmon, J., Timperio, A., McNaughton, S., Thornton, L., . . . Crawford, D. (2012). Cohort
profile: The resilience for eating and activity despite inequality (READI) study. International Journal of
Epidemiology, 42, 1629–1639.
Birch, L., & Davison, K. (2001). Family environmental factors influencing the developing behavioural controls of
food intake and childhood overweight. Pediatric Clinics of North America, 48, 893–907.
Birch, L. L., & Fisher, J. O. (1998). Development of eating behaviours among children and adolescents. Pedeatrics,
101, 539–549.
Croker, H., Lucas, R., & Wardle, J. (2012). Cluster-randomised trial to evaluate the “Change for Life” mass
media/social marketing campaign in the UK. BMC Public Health, 12, 404–418.
Cullen, K. W., Baranowski, T., Rittenberry, L., Cosart, C., Owens, E., Hebert, D., & de Moor, C. (2000). Socioenvironmental
influences on children’s fruit, juice and vegetable consumption as reported by parents: reliability
and validity measures. Public Health Nutrition, 3, 345–356.
Danielzik, S., Czerwinski-Mast, M., Langna¨se, K., &Mu¨ ller, M. J. (2004). Parental overweight, socioeconomic
status and high birth weight are the major determinants of overweight and obesity in 5-7year old children:
baseline data of the Kiel Obesity Prevention Study (KOPS). International Journal of Obesity, 28,
1494–1502.
Department of Health. (2010). Healthy weight, healthy lives: Two years on. London, England: Author.
Fan, S., Pandya-Lorch, R., & Yosef, S. (Eds.). (2014). Resilience for food and nutrition security: An IFPRI 2020
book. Washington, DC: IFPRI.
Fruh, S. M., Fulkerson, J. A., Mulekar, M. S., Kendrick, L. A. J., & Clanton, C. (2011). The surprising benefits of
the family meal. The Journal for Nurse Practitioners, 7, 18–22.
Hammons, A. J., & Fiese, B. H. (2011). Is frequency of shared family meals related to the nutritional health of
children and adolescents? Pediatrics, 127, 1565–1574.
Hubbs-Tait, L., Kennedy, T. S., Page, C. M., Topham, G. L., & Harrist, A. W. (2008). Parental feeding practices
predict authoritative, authoritarian, and permissive parenting styles. Journal of the American Dietetic Association,
108, 1154–1161.
Masten, A. S., & Coatsworth, J. D. (1998). The development of competence in favorable and unfavorable
environments: Lessons from research on successful children. American Psychologist, 53, 205.
McMillan, J., & Reed, D. (1993). Defying the odds: A study of resilient at-risk students. Richmond, VA:
Metropolitan Educational Research Consortium.
Pearson, N., Atkin, A. J., Biddle, S. J., Gorley, T., & Edwardson, C. (2010). Parenting styles, family structure and
adolescent dietary behaviour. Public Health Nutrition, 13, 1245–1253.
Place, M., Reynold, J., Cousins, A., & O’Neill, S. (2002). Developing a resilience package for vulnerable children.
Child Adolescent Mental Health, 7, 162–167.
Rhee, K. E., Lumeng, J. C., Appugliese, D. P., Kaciroti, N., & Bradley, R. (2006). Parenting styles and overweight
status in first grade. Official Journal of the American Academy of Pediatrics, 117, 2047–2054.
Shaw, D.,McMaster, R., & Newholm, T. (2015). Care and commitment in ethical consumption: An exploration of
the “attitude-behaviour gap.” Journal of Business Ethics, 136, 251–265.
Twiddy, M., Wilson, I., Bryant, M., & Rudolf, M. (2012). Lessons learned from a family-focused weight
management intervention for obese and overweight children. Public Health Nutrition, 15, 1310–1317.
Ungar, M. (2008). Resilience across cultures. British Journal of Social Work, 38, 218–235.
Ventura, A. K., & Birch, L. (2008). Does parenting affect children’s eating and weight status? International
Journal of Behavioural Nutrition and Physical Activity, 15. doi:10.1186/1479-5868-5-15.
Wagnild, G. (2009). A review of the Resilience Scale. Journal of Nursing Measurement, 17, 105–113.
Wagnild, G. M., & Young, H. M. (1993). Development and psychometric evaluation of the Resilience Scale.
Journal of Nursing Measurement, 1, 165–178.
Wood, M. (2018). Resilience research and social marketing: the route to sustainable behaviour change. Journal of
Social Marketing, Vol 9(1), pp77-93.
Wood, M., & Shukla, P. (2016). Weight bias, health consciousness and behavioral actions (activities). Eating
Behaviors, 23, 200–205.
Wood, M. and Shukla, P. (2019) ‘Resilience, Parenting Style, and Children’s Eating Behavior’, Social Marketing Quarterly.